In September 2025, 313 Salvadoran men prepared to travel home from the Democratic Republic of Congo. These men had been working in malaria-endemic regions where limited local health resources and inconsistent preventative treatment left them vulnerable to infection. While many remained asymptomatic during their transit, the group represented a concentrated biological threat—a large, mobile population potentially carrying the malaria parasite back to a nation where the disease was no longer a major concern.

César Velásquez Arteaga at El Salvador’s Ministry of Public Health received the names and flight details of the individuals ahead of their arrival. With this information in hand, the Ministry sent a team to screen the men upon their return. On September 7, the first group arrived into El Salvador and all underwent testing and isolation while waiting for lab results. Eight tested positive on arrival but the rest tested negative and were allowed to return home. Because they knew malaria could surface later, officials organized follow-up testing for those that returned home and surfaced an additional five cases, sparking fears that the disease could reemerge in these malaria-free zones and put local communities at risk.
After this initial group of arrivals, hundreds of men continued to arrive on different flights over a period lasting several weeks, placing increased demands on health officials and keeping the threat of malaria alive. As the rest of the group returned home over the next several weeks, the number of cases eventually ballooned to 113, sparking fears that the disease might become endemic once again.

A high-speed, cross-sector coordination strategy helped contain the cases before the men even landed: “We already had a structure available and active to respond,” Dr. Velásquez Arteaga explained. By working together with the Ministry of Foreign Affairs, immigration officials and airlines, Dr. Velásquez’s team was ready to detect any cases by testing the men on arrival, then again at seven, 14 and 21 days. Strong communication between the Ministry of Health and facilities and health care workers at the local level, meanwhile, was critical in mounting an initial response within 24 hours of the first confirmed cases.
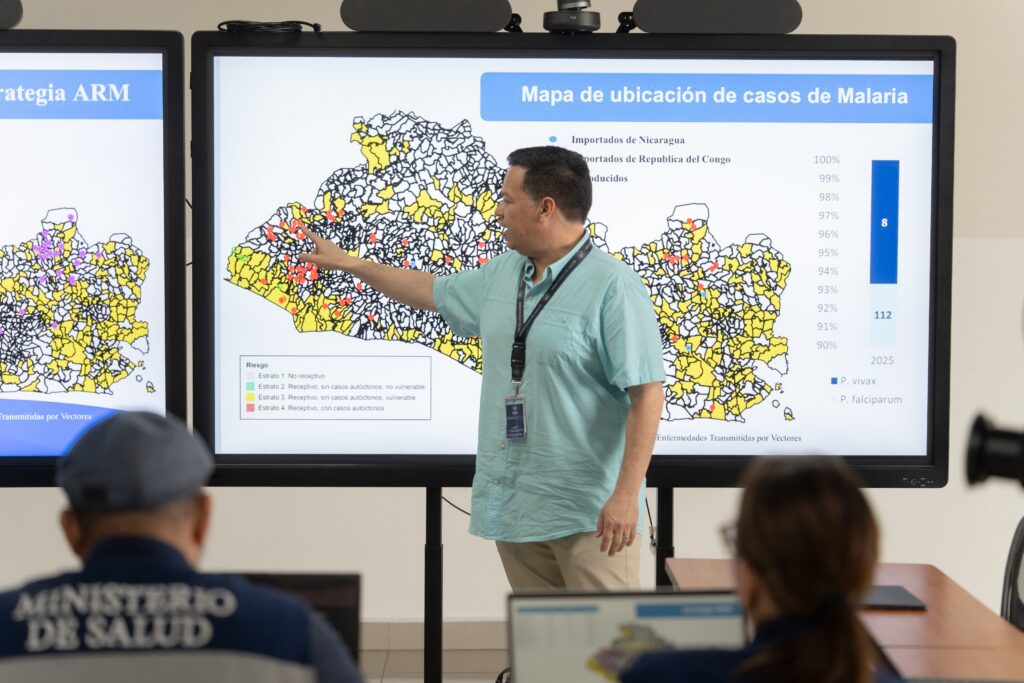
This coordination was maintained through a rigorous daily rhythm. Public health leaders from all five of the country’s regions met every morning for briefings, followed by afternoon national sessions where a real-time, geolocated dashboard tracked critical response metrics including cases, testing, medication administration and local vector control measures.
As the men returned home, cases reached 13 of El Salvador’s 14 departments, which presented a major logistical bottleneck for the distribution of antimalarials. “At the time, we had little medication, so transporting it to each location was difficult for us, and this bottleneck slowed down the administration of medication,” said Dr. Ana Maria Barrientos Llovet at the Ministry of Public Health, who also served as a consultant to the Pan American Health Organization with 7-1-7 Alliance funding.
The Ministry made the strategic decision to capitalize on the country’s geography by centralizing malaria care at a single hospital located in a high-altitude region. Because the malaria-carrying vectors cannot survive at such elevations, this move ensured that patients received supervised, high-quality treatment in a buffer zone where the risk of reestablishing local transmission was effectively zero.
On the ground, local response teams turned individual cases into containment zones. For every confirmed infection, authorities established a five-kilometer “vector control perimeter” involving fumigation and distribution of insecticide-treated bed nets. Within a tighter one-to-two-kilometer radius, community health promoters conducted active surveillance, testing the entire population within the established perimeter to ensure the parasite hadn’t jumped from the travelers back to the community.

Finally, to manage the sudden surge of nearly 100,000 tests, the Ministry overhauled its diagnostic infrastructure by establishing a dedicated 24-hour collection and testing center, allowing them to clear a massive backlog and ensure prompt diagnoses within 24 hours. This round-the-clock laboratory, combined with mandatory treatment for anyone returning to El Salvador from DRC, successfully halted the outbreak.
By the time the team concluded its response efforts, not a single secondary case had been recorded beyond the 113 cases among the initial group of travelers, and the outbreak was stopped with no reported deaths.

Early detection using health screening and blood tests

24-hour laboratory to process the surge in samples

Vector control interventions in residential areas